Too Many Kids With Sickle Cell Disease Aren't Getting Appropriate ...
by Ashaunta Anderson, MD, MPH, MSHS August 26, 2024
Anderson is a pediatrician.
I was cradling my newborn son in my kitchen when I got the call from his pediatrician in winter 2015.
"Are you sitting?" he asked somberly.
I sank slowly into a chair knowing what he was about to share. My 2-week old had tested positive for sickle cell disease, a life-threatening genetic condition that causes painful joints that feel like broken bones and creates blockages in the brain, making sickle cell a leading cause of stroke in children.
Sickle cell disease is a genetic condition that affects an estimated 100,000 individuals in the U.S., occurring in about one in 365 African American births and in about one in 16,300 Hispanic American births. I studied sickle cell disease as a medical student at the NIH and was aware of what lay ahead for my son and our family.
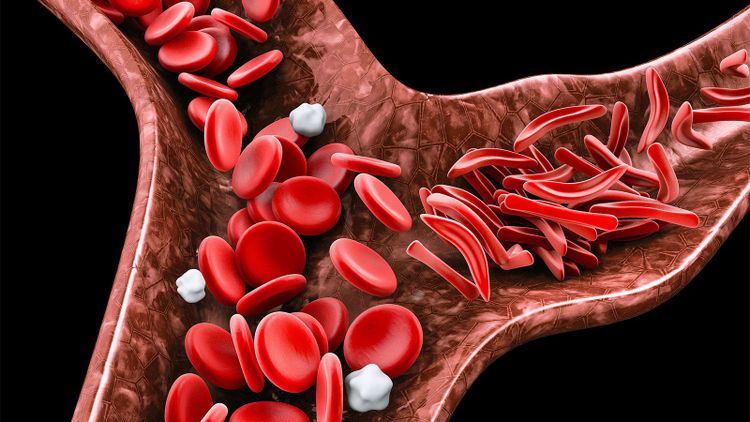
It is a devastating diagnosis. The condition makes the red blood cells more likely to stick together and block blood flow when oxygen levels are low. Essentially any body part can be affected, but the clinical hallmark of sickle cell disease is severely painful joints. The spleen is particularly affected because its main jobs are to process damaged red blood cells and to protect against certain kinds of bacteria. Repeat blockage of blood flow in the spleen leaves a child vulnerable to rapidly progressive bacterial infections. Similar blockage of blood flow in the brain causes stroke.
These well-known symptoms have inspired innovative research and therapies, such as the recent FDA approval of gene therapies for patients ages 12 years and older with sickle cell disease. However, significant risk associated with attempts at cure remain, leaving preventive measures as the mainstay approach: twice-daily doses of antibiotics, such as penicillin, can protect children against life-threatening infections, and annual brain ultrasounds can identify children at high risk of stroke, a danger that can be reduced with blood transfusions.
This is why I was shaken when the study I led revealed that many children with sickle cell disease are not receiving the preventive care recommended to reduce the sicknesses and life-threatening disabilities from the most common form of sickle cell disease, sickle cell anemia.
Our research team studied Medicaid claims data between 2010 and 2019 from two states -- California and Georgia -- and the findings were alarming. We found that just one in five children between 3 months to 5 years old with sickle cell anemia -- in a patient population that was 90% African-American -- received daily antibiotics to prevent infections. And only about half of children and adolescents between ages 2 and 15 underwent a yearly brain scan to assess their stroke risk. Evaluations in several other states produced similar results.
The new data beg a perplexing question: Why aren't these children receiving essential preventive care?
Our study unexpectedly found that low-income children on Medicaid with sickle cell anemia were more likely to receive antibiotics if they lived in rural Georgia than if they lived in urban areas. Data trends also suggested that patients had a greater chance of receiving preventive antibiotics if their doctor was a pediatric hematologist instead of a general pediatrician. Finally, we found there was also a lower probability a patient would receive an annual scan for stroke as they got older.
Limited access to hospitals and clinics that can perform brain ultrasounds and a lack of money and transportation can prevent a family from refilling a penicillin prescription every 2 weeks. Privately insured children with sickle cell are more likely to obtain care to keep them healthier.
I also contend that race is a factor, because sickle cell disease primarily affects African Americans. I had a patient's mother turn down therapy for her child because her grandfather was a participant in the infamous Tuskegee study that allowed African Americans to go without treatment for syphilis. Other studies have described inadequate pain management for African Americans -- a failing of a healthcare system that patients of color avoid because they feel they have been treated poorly. This painful history makes it more likely that a patient will not take potentially life-saving antibiotics or navigate a tertiary care center for an ultrasound screen.
After I had my second child and received that same disheartening phone call from that same pediatrician, I went into an outright free fall. My daughter's hospitalization at just 9 weeks old haunts me still. We are well -- all of us -- and I am thankful for that. I am thankful for the kind and knowledgeable clinicians who have helped keep us that way.
More education for pediatricians, pediatric hematologists, and families can help fill deficiencies in preventive care. Medicaid can add these preventive measures to the program's core set of quality benchmarks required of public programs nationwide. This can improve health outcomes by mandating institutions track performance and by financially incentivizing them to meet quality benchmarks.
By instituting tailored quality improvement programs in every clinic and hospital, we can deliver better care for children with sickle cell anemia to keep them healthier for longer. Such programs can offer help with transportation costs for patient appointments and simplify the prescription refilling process by having medication sent to homes. Community health workers can also check in with families and help with prescription management and with scheduling transcranial ultrasounds, as well as assist with other social determinants of health needs, such as housing and food insecurity.
Our research team is hoping to continue researching preventive care in more states in order to prompt change. The deficient performance rates in our study, coupled with future investigation, must be viewed as a call to action toward rightful expectations of high-quality care in pediatric sickle cell disease.
Ashaunta Anderson, MD, MPH, MSHS, is a pediatrician with Children's Hospital Los Angeles.







































